Guide To Manage Functional Constipation In Pediatric Patients
Division of Gastroenterology, Hepatology, Pancreatology and Nutrition
Children meet the Rome IV definition of functional constipation if they have at least two of the following:
- Two or fewer defecations per week
- Excessive stool retention
- Painful or hard bowel movements
- Large diameter stools
- Large fecal mass in the rectum
Toilet trained children:
- Soiling at least once a week
- Large diameter stools which clog the toilet
Children more than 4 years of age:
- 2 or fewer defecations per week
- At least 1 episode of soiling per week
- Retentive posturing/stool holding
- Painful or hard bowel movements
- Large fecal mass in the rectum
- Large diameter stools which clog toilet
- Symptoms can’t be explained by another condition
What are the red flags?
- History of delayed passage meconium (more than 48 hours after birth)
- Failure to thrive
- Severe abdominal distention
- Perianal fistula
- Absent anal wink
- Sacral dimple
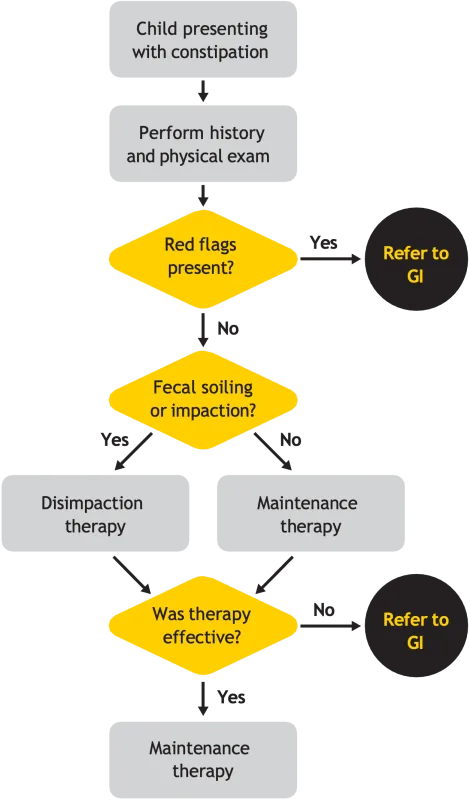
Medical therapies for fecal disimpaction at home
| Route | Therapy | Dosing |
|---|---|---|
| Oral | Polyethylene glycol 3350 mixed as 17 g/8 oz of water, juice, or other liquid | Over 3 years of age: 1–1.5 g/kg per day for 3 days, may be continued for up to a week. A large daily dose of up to 100 g/d for 1–2 days; lower doses for longer periods, up to 12 weeks, have been used. |
| Oral | Magnesium citrate | 4 mL/kg per day – generally given on 2 consecutive evenings |
| Oral | Lactulose | 1 mL/kg, twice a day, for up to 12 weeks then tapered over 4 weeks |
| Rectal | Normal saline enema | 10 mL/kg, generally given on 2–3 consecutive evenings |
| Rectal | Sodium phosphate enema | Over 12 years of age: 4.5 oz. enema on 2–3 consecutive evenings 5–11 years of age: 2.25 oz. on 2–3 consecutive evenings 2–4 years of age: 1 oz. on 2–3 consecutive evenings |
| Rectal | Mineral oil enema | Over 12 years of age: 4.5 oz. on 2–3 consecutive evenings 2-11 years of age: 2.25 oz. on 2–3 consecutive evenings |
| Rectal | Biscodyl suppositories | 1–2 suppositories per day for 2–3 consecutive evenings, may be repeated in 1–2 wk |
Note that systematic dosage and safety studies on these medications have not been rigorously performed in the pediatric age range. Adapted from Colombo JM, Wassom MC, Rosen JM. Constipation and encopresis in childhood. Pediatr Rev. 2015:36(9)-392-401. (10)
Maintenance therapy for chronic constipation
| Therapy Type | Therapy | Dosing |
|---|---|---|
| Osmotic laxatives | Polyethylene glycol 3350 | 0.5–1.5 g/kg per day |
| Osmotic laxatives | Lactulose | 1–3 mL/kg per day in 2 divided doses |
| Osmotic laxatives | Magnesium hydroxide | Less than 2 years of age: 0.5 mL/kg per day 2–5 years of age: 5–15 mL/day (before bedtime or divided) 6–11 years of age: 15–30 mL/day (before bedtime or divided) Over 12 years of age: 30–60 mL/day (before bedtime or divided) |
| Stool softeners/lubricants | Docusate | 5 mg/kg per day (400 mg maximum) |
| Stool softeners/lubricants | Mineral oil | 1–3 mL/kg per day divided into 2 doses |
| Stimulant laxatives | Senna | 1–2 years of age: 2.2–4.4 mg/day as 1 or 2 divided doses Over 2–6 years of age: 4.4–6.6 mg/day as 1 or 2 divided doses Over 6–12 years of age: 8.8–13.2 mg/day as 1 or 2 divided doses Over 12 years of age: 17.6–26.4 mg/day as 1 or 2 divided doses |
| Stimulant laxatives | Bisacodyl | 3–12 years of age: 5–10 mg/day Over 12 years of age: 5–15 mg/day |
| Chloride channel activators | Lubiprostone Prucalopride | New prescription medications approved only for adults with very limited pediatric (off-label) experience |
| Chloride channel activators | Linaclotide | Over 6 years of age: 72 mcg/day |
Adapted from Colombo JM, Wassom MC Rosen JM. Constipation and encopresis in childhood. Pediatr Rev. 2015,36(9)-392-401. (10)
Other recommendations
- Have child sit on toilet when they first wake in the morning and after every meal. This is when the colon is most active. This is especially important for those children with soiling.
- Child should have a step stool below their feet to assist in defecation. They should sit upright and should not cross or stiffen their legs.
- Ensure they are drinking plenty of water. Goal of about 1 oz. per body weight in kilograms per day.
- Do not punish for stool accidents — this is rarely on purpose. If having accidents need to do a disimpaction.
- Consider providing small rewards for complying with toilet sitting (for example, a sticker chart.)
- Have the family watch “The Poo in You” video from University of Colorado on YouTube. Another great video is Constipation in Children: Understanding and Treating this Common Problem on YouTube from Primary Children’s Hospital in Utah.
- Constipation Care package from GIkids.org is an excellent resource for patient education. It includes a stool diary.
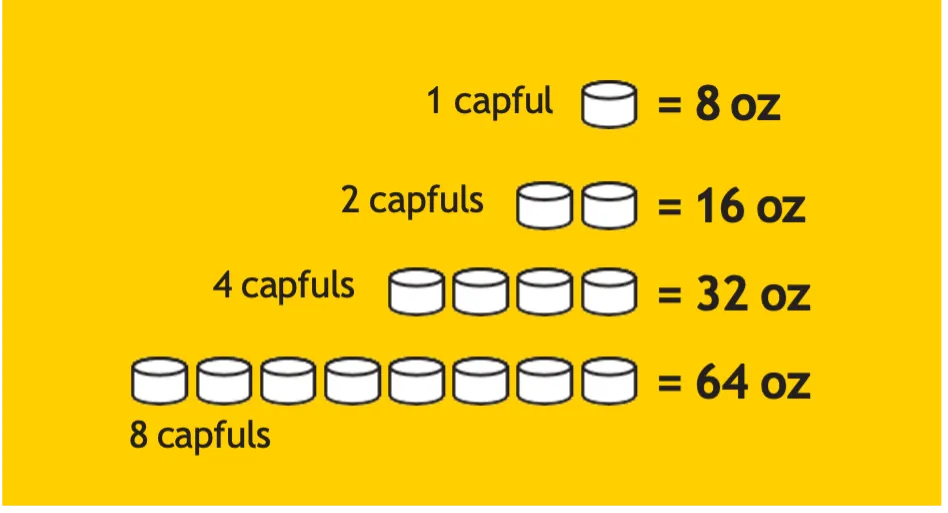
Mixing MiraLAX®
- Sometimes mixing with lukewarm water helps it dissolve.
- A larger volume can be mixed and then kept in the refrigerator.
- Mix with water and then add flavoring (such as flavor drops)
- For an easy calculation for dosing: divide weight in kg by 4. This equals the volume in oz. they need for each dose For example: a 20 kg child would need 5 oz. 3 times a day for disimpaction (~1.5 g/kg) and 5 oz. 2 times a day for maintenance (~1 g/kg).
Common questions
MiraLAX is a stool softener that helps bring more water back into the stool. The body will not “get used to it”. Higher doses may be needed due to changes in diet, fluid intake, activity, and stool holding. It does not affect the function of the nerves in the gut and make them weaker.
Soiling typically occurs when a child has been stool holding and liquid stool started leaking around a stool impaction in the rectum. Many families will tell you the soiling will stop for a day or two if the child passes a large hard stool.
Yes. There is no evidence that using stool softeners for prolonged periods will cause long term side effects.
A well rounded diet should not cause constipation. However, a diet heavy in processed foods, especially starch heavy (like white bread and white rice) can exacerbate constipation. High fat foods and drinks will also slow down gut motility and may predispose to constipation. Drinking excessive amounts of milk can also exacerbate constipation (due to the fat).
Xrays are not recommended to diagnose constipation in most cases. History and physical exam is all that is needed.
Rarely do blood tests find a cause (thyroid, celiac).
No. Constipation will also not cause the colon to rupture nor does it cause bad breath. It may, however, predispose to urinary tract infections, decreased appetite, and stomachaches.
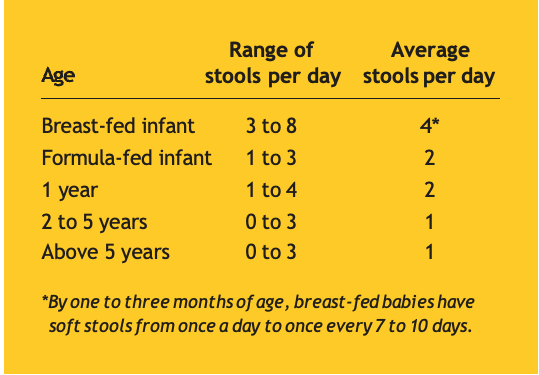
See the chart below.
Bristol Stool Chart

Separate hard lumps, like nuts (hard to pass)

Sausage-shaped, but lumpy

Like a sausage, but with cracks on its surface
Like a sausage or snake, smooth and soft
Soft blobs with clear-cut edges (passed easily)
Fluffy pieces with ragged edges, a mushy stool

Watery, no solid pieces. Entirely liquid