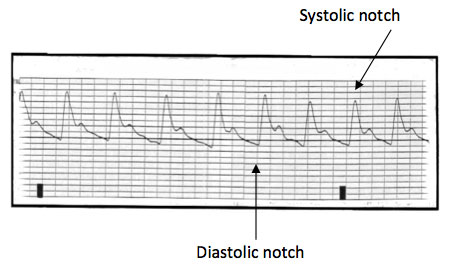
Arterial blood pressure monitoring
- Invasive way to monitor blood pressure more accurately.
- Ensure waveform is appropriate before interpreting pressures. BP can be artifactually low or high.
- Pay attention to pulse pressure. Wide pulse pressure: Chronic anemia, PDA, vasodilatation. Narrow pulse pressure: Status asthmaticus, Cardiac tamponade, dehydration
- Use heparinized normal saline to prevent clotting @ 1-2 cc/hr.
- Add papaverine 30-60 mg to heparinized fluids to help with vasospasm.

Central venous pressure monitoring
- CVP reflects the amount of blood returning to the heart (preload).
- Normal CVP tracing has 3 positive waves (a,c,and v) and 2 negative waves (x and y). The a wave is caused by atrial contraction, c wave by ventricular contraction against a closed tricuspid valve, and the v wave is caused by atrial filling. The x descent is due to tricuspid valve being pulled away from the right atrium by contracting ventricle, while the y descent occurs as tricuspid valve opens and blood enters the ventricle.
- Normal CVP: 2-6 mmHg
- Ensure CVP reading is obtained with appropriate leveling and at end expiration.
High CVP: TR, TS, heart failure, elevated intrathoracic pressure
Low CVP: Hypovolemia and distributive shock (anaphylaxis) - Use heparinized normal saline fluids @ 2-3cc/hr to prevent clotting.

Cerebral & renal somenetics
- Measures tissue perfusion and oxygen delivery by infrared spectroscopy
- Helpful to assess trends and adequacy of cardiac output
- Useful for post op hearts and children in shock
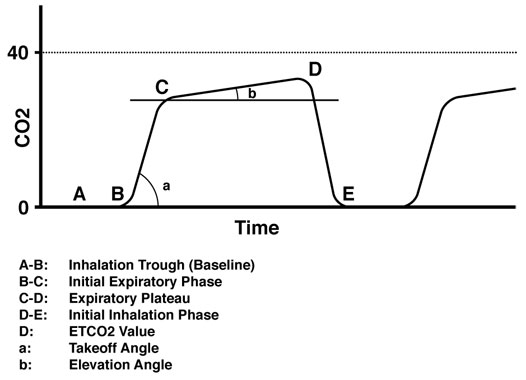
End tidal CO2 monitor
- Monitor CO2 level when mechanically ventilated without drawing blood gases
- Need to ensure that the level does correlate with a blood gas initially!
- Helps to detect dead space ventilation/ET tube obstruction
- ***Unreliable in presence of air leak!!!

Pulse oximetry
- Monitors systemic oxygen saturation
- Needs adequate tissue perfusion to be reliable
- Ensure good waveform before interpreting the saturation
- Unreliable in CO and Met Hb poisoning (low PaO2 with normal sat)
- Inability to pick up sats suggests decreased tissue perfusion
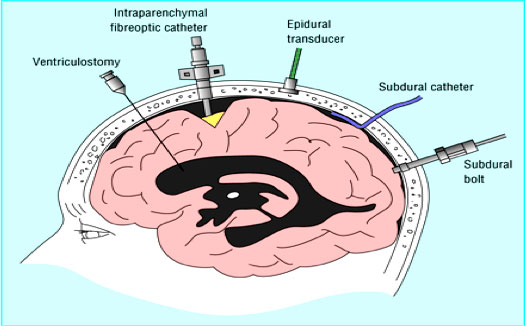
ICP monitoring
- Indicated in patients with concerns about elevated intracranial pressure
- Normal ICP:0-10 mmHg, ICP > 20 is abnormal and needs to be treated
- Ensure device leveled accurately
- Ensure good waveform before interpreting and reacting to pressures
- ***Pressure spikes that go up and stay up are of most concern and need treatment!
- Different devices available as shown in picture (subdural bolts and ventriculostomy are most common in our PICU)
- Cerebral perfusion pressure (CPP) = Mean arterial pressure (MAP) – ICP Goal is > 50 for infants, > 60 for most children, > 70 for adults
Telemetry
- Continuous ECG monitoring allows for assessment of heart rate and rhythm, ischemia and conduction defects