Preparing for anterior urethral stricture disease treatment
Anterior urethral stricture disease is a narrowing in the anterior urethra. The anterior urethra is a tube that goes from the prostate to the tip of the penis. It carries urine (pee) and semen out of the body.
This guide explains:
- Causes and symptoms of anterior urethral stricture disease
- What you can expect when you are diagnosed
- What to expect with treatment
Lower urinary tract symptoms
These are most commonly:
- Slow urine flow
- Urine dribbling
- Urinary retention (not able to empty the bladder
Symptoms can also be:
- Urinary urgency and frequency (having to urinate [pee] often and on short notice)
- Pain or burning with urination
Urinary tract infection (UTI)
UTIs are more common in men who cannot fully empty their bladder. UTIs can cause
- Painful urination
- Cloudy or smelly urine
- Sometimes fevers and body chills
In severe cases, the infection can involve the kidneys. If this happens, you will be hospitalized and given antibiotics through an intravenous (IV) catheter.
Bladder dysfunction
The bladder muscle can thicken if the stricture is not treated in time. Thickening of the bladder muscle can lead to an increase in urine symptoms. Over time, the bladder wall weakens and bladder size increases. In the end, you may not be able to empty your bladder.
Kidney dysfunction
This can happen if:
- Urine backs up into the kidney
- The pressure in the bladder is too high
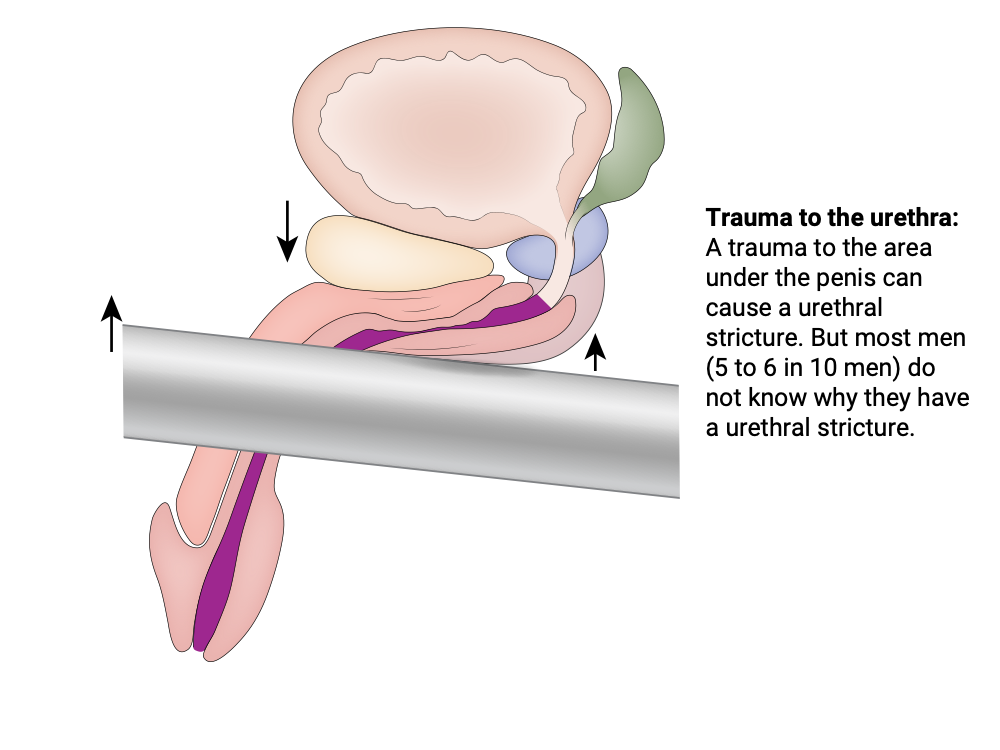
Most men (5 to 6 in 10 men) with urethral stricture disease do not know why they have the condition. In other men, the stricture is caused by:
- Infection or sexually transmitted disease (1 in 10 men)
- Trauma to the urethra (2 in 10 men)
- A congenital (present from birth) or pediatric condition (1 to 2 in 10 men)
In most cases, people choose to be treated when urinary symptoms are severe. The most common symptoms that lead to treatment are recurrent UTIs and urinary retention. Treatment is sometimes needed because of kidney damage.
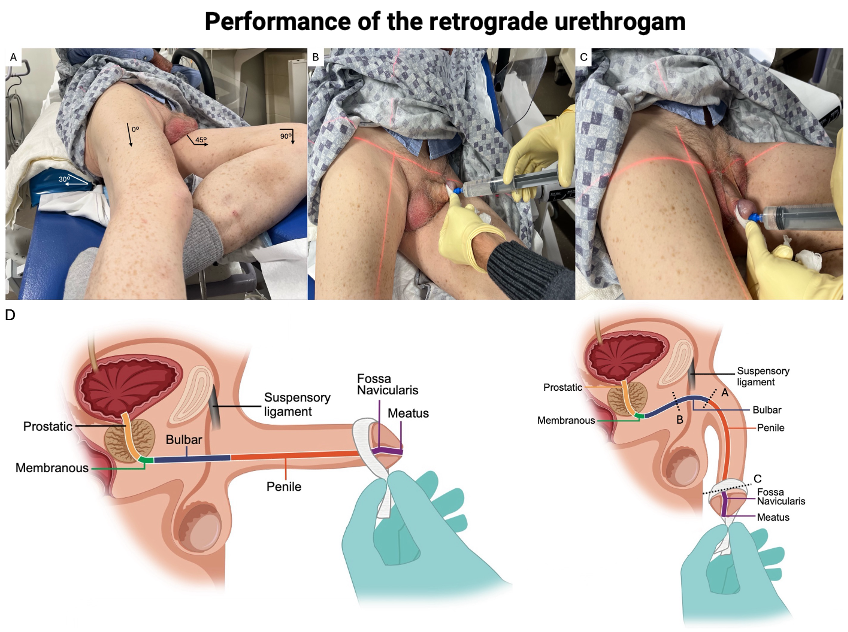
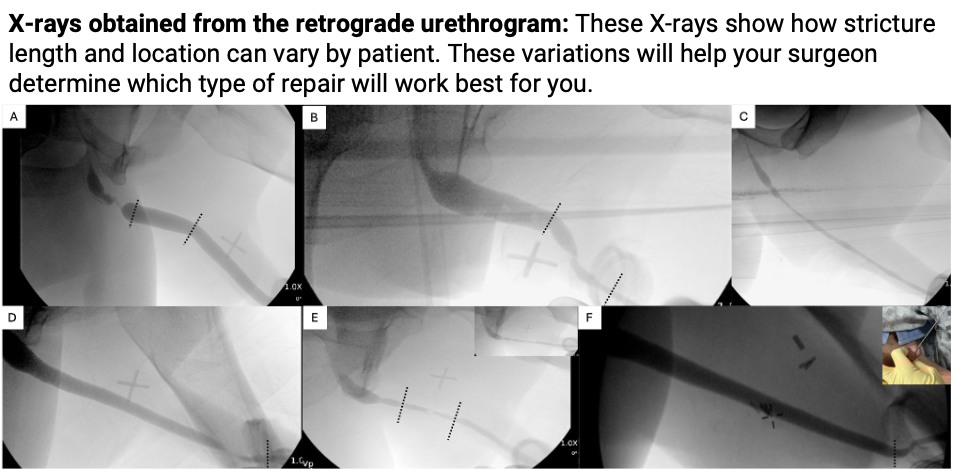
Retrograde urethrogram (RUG): Retrograde urethrogram is an X-ray of the urethra. X-ray dye (also called contrast) is injected into the urethra before the X-ray is taken. The X-ray images show the location, length, and severity of the stricture. It can help you and your surgeon pick the right treatment option.
Uroflowmetry: Uroflowmetry measures the flow of urine (how quickly you empty your bladder, how much urine comes out, and how long it takes). You will need to come to your appointment with a full bladder. You will urinate into a device that measures the flow in milliliters (mL) per second.
Post-void residual: An ultrasound device is placed on your lower abdomen (belly). It measures how much urine stays in your bladder after you urinate.
There are no medical treatments for anterior urethral stricture disease. If you have urethral stricture disease with lichen sclerosus (a rare skin disease that causes itchy, white patches on the genitals), your urologist may offer you a topical steroid (clobetasol). This steroid helps with some of the itching and irritation on the tip of the penis.
Endoscopic procedures are minimally invasive treatments for urethral stricture disease. The surgeon uses a cystoscope (tool to see into the bladder). It has a thin tube with a light and a tiny video camera on the end.
Minimally invasive treatments open the urethra to improve urination. They will not remove the scar tissue. The most common minimally invasive treatments are urethral balloon dilation and direct visual internal urethrotomy. In both procedures, medicine is injected into the urethral stricture. This lowers the risk of the stricture coming back.
These procedures can be done in the clinic while you are awake, with medicine to numb the urethra. They can also be done in the operating room while you are under general anesthesia.
The location and type of anesthesia will depend on your comfort and the length and location of the stricture. Both procedures start with the placement of a wire through the stricture.
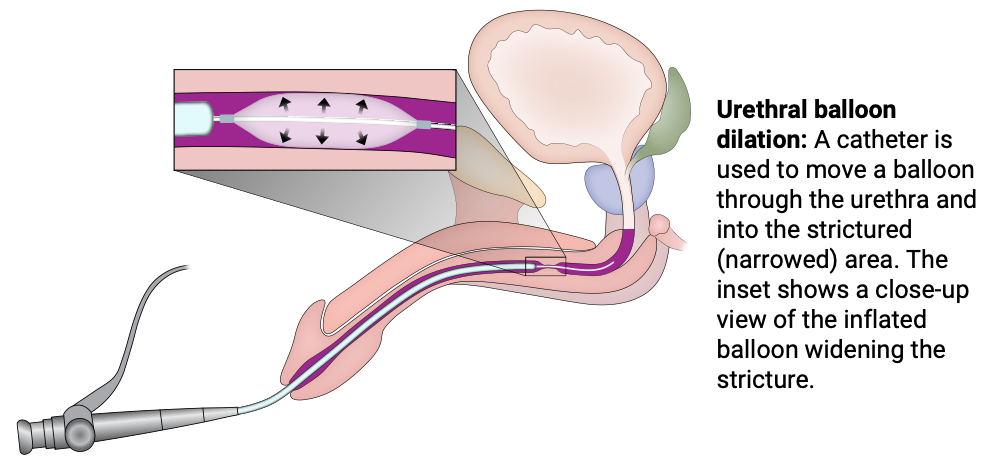
Urethral balloon dilation
A small catheter with a balloon port is advanced over the wire. The balloon is then inflated, and the stricture is dilated. A catheter is then placed over the wire. It stays in place for 48 to 72 hours. In some men, we use a newer balloon that is coated with a medicine that decreases scar reformation. This balloon is called Optilume®.
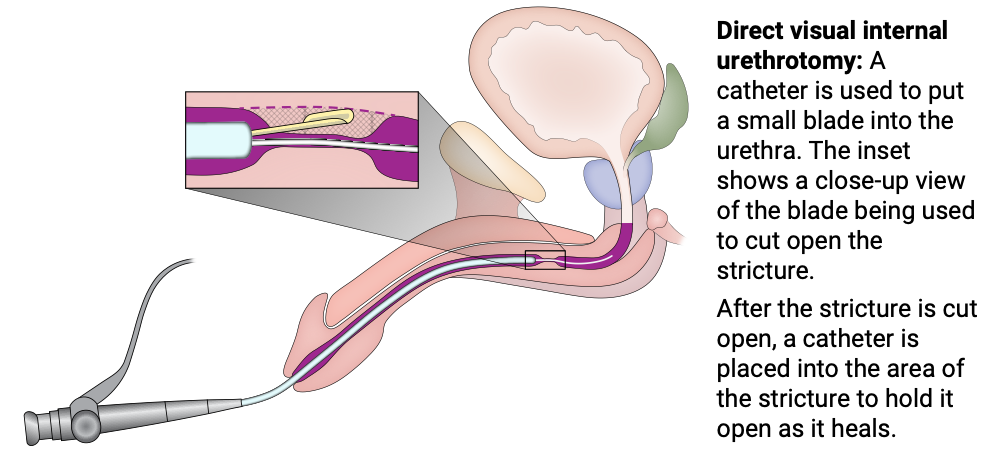
Direct visual internal urethrotomy (DVIU)
An instrument with a small blade is put into the urethra. The blade cuts open the strictured (narrowed) area. A catheter is then placed over the wire. It stays in place for 48 to 72 hours.
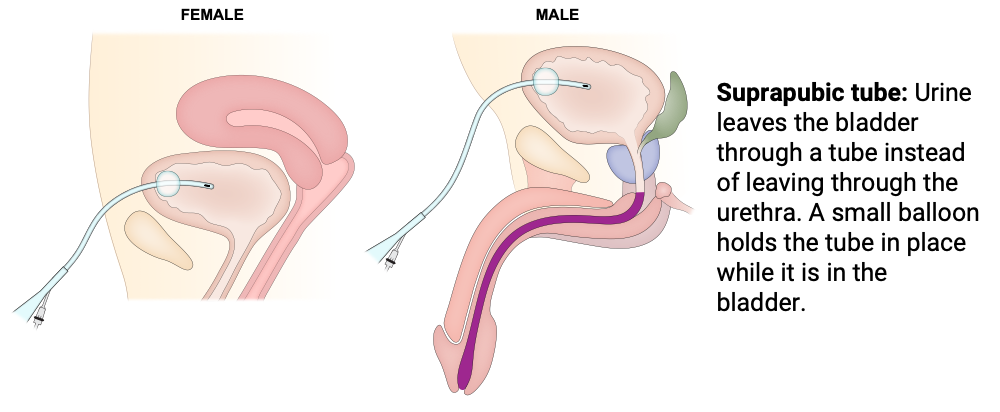
Suprapubic tube
In some situations, a suprapubic tube can be placed into the bladder. This bypasses the urethral stricture and allows for direct drainage of urine from the bladder.
A suprapubic tube can be a permanent solution if the stricture cannot be treated, or it can be a temporary solution while waiting for urethroplasty surgery.
Two business days before your procedure, UI Health Care will contact you with information about when and where to arrive for your operation.
On the day of the procedure, you will meet with the anesthesiologist and the urology team. You will agree on a final plan for surgery.
The surgery will be done with a cystoscope. There will be no incisions in the skin.
The procedure often lasts 30 to 60 minutes. In most cases, the patient can go home on the day of surgery. If there are concerns about bleeding or pain, we will arrange an overnight admission.
Complications right after an endoscopic procedure can be:
Hematuria (blood in the urine)
Dilating or cutting a stricture can lead to blood coming from the tissue under the stricture. In nearly all cases, this bleeding is managed with the urethral catheter. Most of the blood will be seen around the catheter. It may look crusted. In rare cases (less than 1 in 100 patients), a 2nd procedure is needed to stop the bleeding.
Pain
The urethral catheter causes most of the pain after an endoscopic procedure. Your urology team can give you medicine (oxybutynin/Ditropan) at the time of discharge to help with pain.
Nerve injury
In some cases (less than 5 in 100 patients), you may wake up from anesthesia with numbness or tingling in your arms and legs. This is due to the positioning of the legs and arms and the anesthesia. In nearly all cases, this numbness and tingling goes away in 24 to 48 hours.
Infection
We lower the risk of infection by:
- Operating on men who do not have an active infection
- Giving antibiotics at the time of the procedure
A UTI can happen in some men (2 to 3 in 100 men). Infections often result in pain or redness around the incision, or cloudy or smelly urine in the catheter.
About half of patients that get a minimally invasive endoscopic procedure are cured. The rate is higher in patients who have:
- Short strictures (less than 1 centimeter)
- No previous endoscopic procedures (dilations or incisions) of the stricture
- A stricture located closer to the sphincter (proximal bulbar stricture) rather than a stricture in the penile urethra
- Steroids or other medicines after the stretching or incision of the stricture
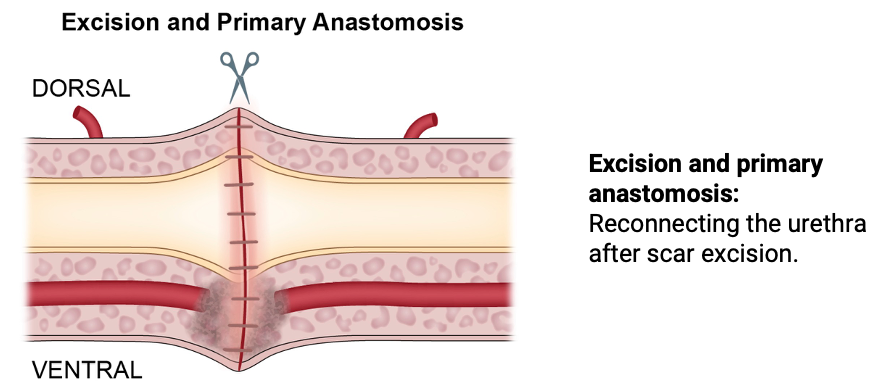
The gold standard surgical treatment for urethral stricture disease is an anterior urethroplasty. In this procedure, the strictured (narrowed) part of the urethra is either excised (removed) or augmented (made larger by adding grafted tissue).
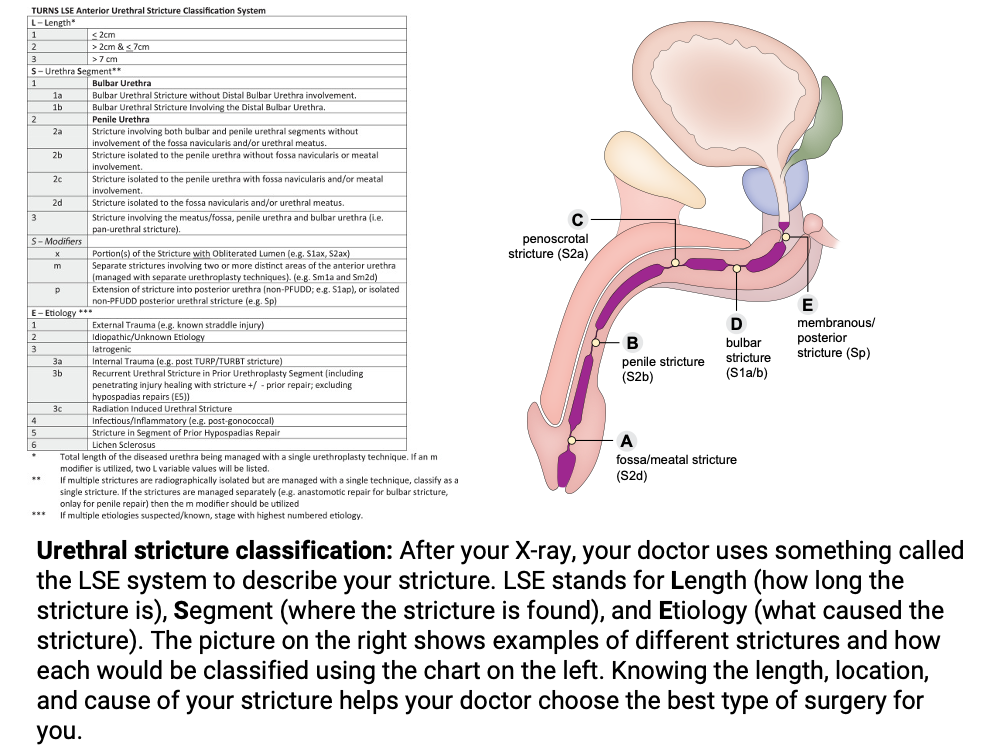
The type of surgery will depend on the length and location of your urethral stricture as determined by the X-ray of your urethra (retrograde urethrogram). Your surgeon will then classify and stage your urethral stricture to give you the most likely type of repair that will need to be performed and their expected outcomes.
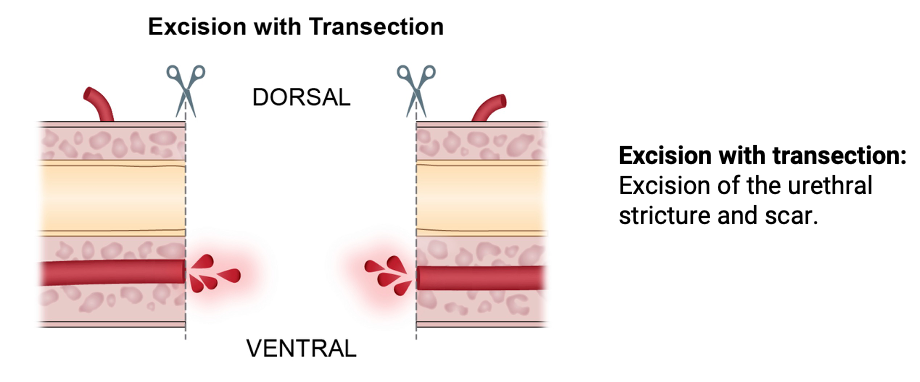
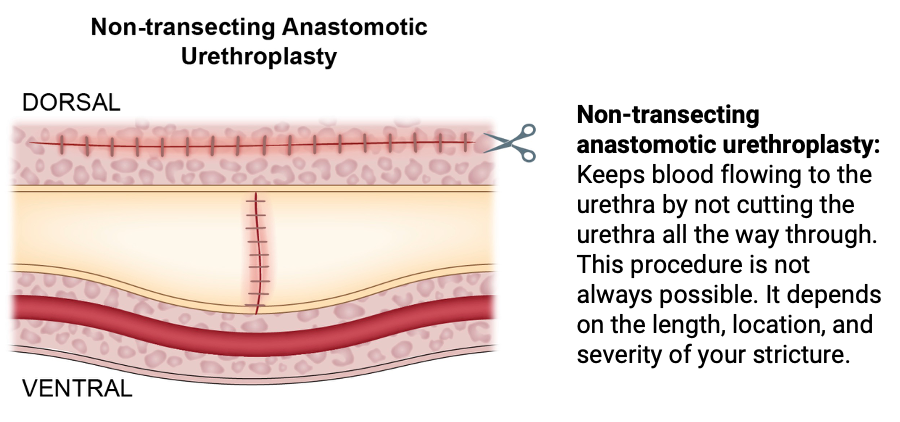
Excising the stricture can be done using 2 techniques:
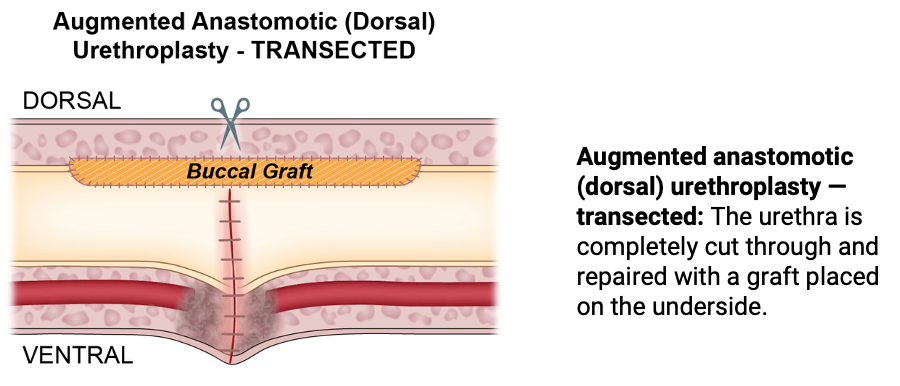
- Transecting (cutting the spongy tissue in half)
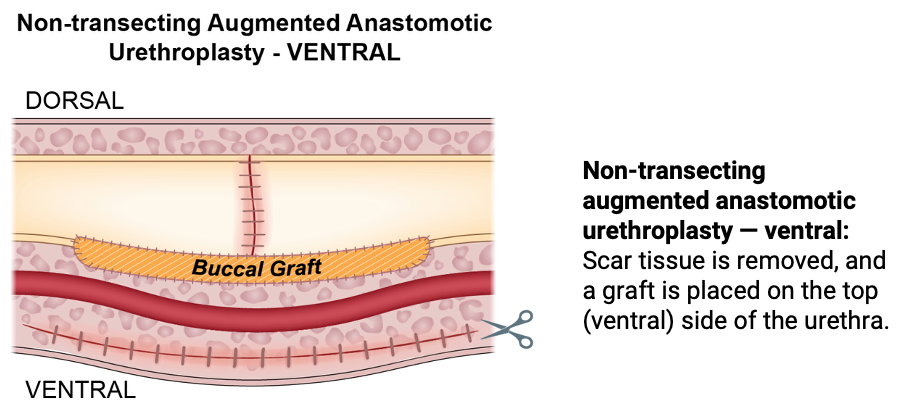
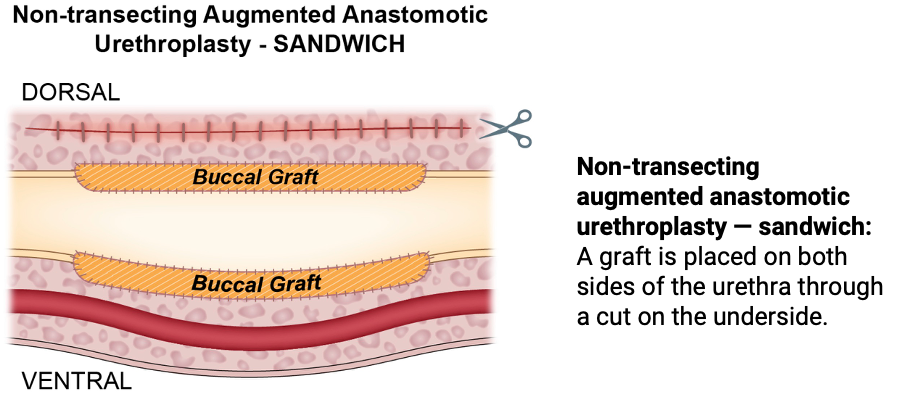
- Nontransecting (preserving the spongy tissue)
The decision is often made during the operation, after the surgeon evaluates the health of the tissue.
Ways to excise the stricture
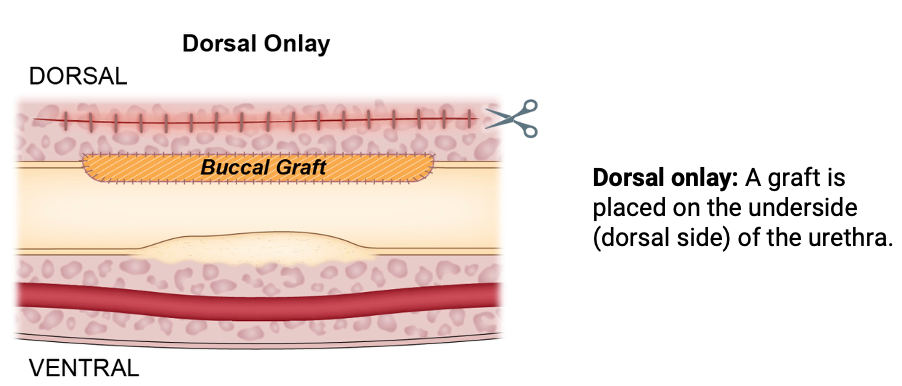
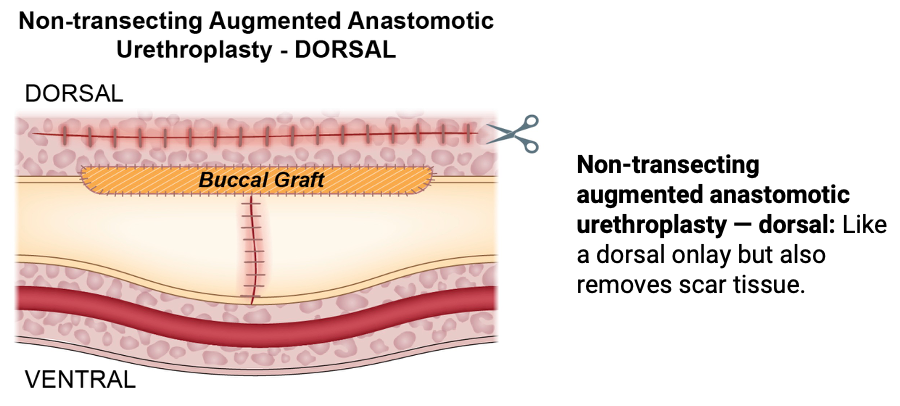
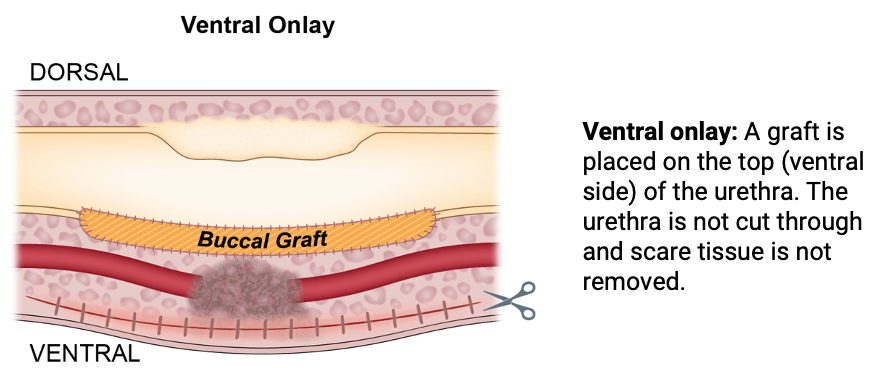
When the stricture is augmented, the opened urethra is often repaired and made larger with tissue called buccal mucosa that is taken from the mouth.
These treatments are used when a stricture that cannot be fixed with an excisional or anastomotic repair. The final treatment is chosen during surgery by your surgeon. They decide based on how the urethra looks and what will give you the best chance for a long-term fix.
Ways to augment the stricture
Two business days before your procedure, UI Health Care will contact you with information about when and where to arrive for your operation.
On the day of the surgery, you will meet with the anesthesiologist and the urology team. You will agree on a final plan for surgery and sign the consent form.
During the procedure you will be in high lithotomy position. A perineal incision will be made for a bulbar stricture. For penile urethral strictures, a penile incision will often be made.
The procedure often lasts 2 to 3 hours. In most cases, the patient can go home on the day of surgery. If there are concerns about bleeding or pain, we will arrange an overnight admission. Patients that need buccal mucosa harvest for their repair are more commonly admitted overnight.
Complications after anterior urethroplasty can be:
Bleeding
The procedure does not end until we manage all bleeding. Delayed bleeds can happen. They can lead to bruising of the area around the incision. Sometimes delayed bleeds also cause blood to come out around, or in, the catheter. In most cases this bleeding will stop on its own.
Pain
Most pain after surgery comes from having the urethral catheter in place. Your care team can give you medicines (oxybutynin/Ditropan) at discharge to help with pain. The incision pain is often mild. It can be controlled with hot or cold compresses.
Nerve injury
In some cases (less than 5 in 100 patients), you may wake up from anesthesia with numbness or tingling in the extremities. This is related to the positioning of the legs and arms and the anesthesia. In nearly all cases, this numbness and tingling goes way within 24 to 48 hours.
Infection
We lower the risk of infection by operating on men who do not have an active infection. We also give you antibiotics at the time of the procedure. An infection of the surgical incisions or in the urinary tract can happen in some men (2 to 3 in 100 men). Infections often result in pain or redness around the incision, or cloudy or smelly urine in the catheter.
Catheter
An indwelling catheter (drains urine from your bladder into a bag outside your body) will be left in place for 2 to 3 weeks. When the catheter is removed, we will do a RUG to make sure the urethra has healed the right way. The catheter can be attached to an overnight bag or a leg bag. You will be given both before you go home.
Wound care
The skin incision is closed with absorbable sutures. You will see the sutures on your skin.
Your surgical team will send you home with a topical antibiotic (bacitracin). It should be put on the incisions 2 times each day for 1 week.
The sutures will start to fall out in about 2 weeks. They may stay in place for up to 1 month. After 10 days, you can use a washcloth in the shower or bath to help loosen the sutures. That will speed up the removal process.
Activity
You should walk right away after surgery. You can go back to all normal activities (if they do not cause discomfort) after your urethroplasty. There are some exceptions:
- No bike riding or other activity that puts pressure on the incision for 1 month.
- No heavy lifting (greater than a gallon milk jug) for 2 weeks. After 2 weeks, you can do heavy lifting and more strenuous physical activities (if they do not cause discomfort).
- No swimming in a pool or hot tub for 1 month.
Pain control
You will be discharged with 3 days of narcotic pain medicine. Take these only if you need them. Alternatives to narcotics are:
- Ibuprofen
- Tylenol
- Hot or cold compresses
Antibiotics
Before the surgical incision is made, you will get antibiotics. You will also get a prescription for an antibiotic. Start taking the antibiotic the night before you are scheduled to have your catheter removed. This helps lower the risk of a UTI.
Clinic visits
First postoperative visit: At your 1st clinic visit after surgery, we will do a RUG to make sure your urethra has healed. Start antibiotics the night before this visit.
Second postoperative visit: If the catheter was removed at the 1st postoperative visit, we will schedule your 2nd visit 3 months after surgery. At this visit, we will do a cystoscopy. A cystoscope is placed into the urethra. This lets the doctor see if the repaired urethra is healing the right way.
Third postoperative visit: The final visit will take place 1 year after surgery. At this visit, we will do a uroflowmetry test. If you are urinating well and the uroflowmetry study shows an adequate urine flow, no further testing is needed. If we are worried about the urethra narrowing again, we may do a cystoscopy.
Future visits
If the urethroplasty is successful at 1 year, very few people have their stricture come back again later. If you see a slowing of your urinary stream or have urinary symptoms again (like the symptoms you had before your urethroplasty) please call our office to set up an appointment.